
Home » Supported Research » Multimodal registration of the brain’s cortical surface
Multimodal registration of the brain’s cortical surface
Title: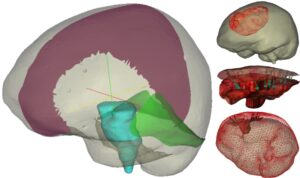
Multimodal registration of the brain’s cortical surface
Project Number:
5R01NS049251-12
Contact PI/Project Lead:
Michael Miga
Award Organization:
National Institutes of Health
Abstract:
With respect to the presenting patient population, approximately 69,720 new cases of primary brain tumors are expected to be diagnosed in 2013 with approximately 35% of those tumors being malignant. Brain tumors are the second leading cause of cancer-related deaths in children under age 20, and males between the ages of 20-30. Interestingly, incidence rates are significantly higher in developed countries, approximately 70% higher. Five year survival rates following diagnosis of a primary brain tumor is approximately 33.8% on average but vary considerably with age (e.g. over the age of 65 is 10%). According to the National Cancer Institute surgical removal is the recommended treatment for most brain tumors with the goal of the most complete resection possible while preserving neurological function. With respect to the mission of the National Institute for Neurological Disorders and Stroke, more complete resection reduces the burden of neurological disease by restoring function, extending life, and improving the quality of that life. With respect to surgical therapy, the deployment of visual displays that relate the patient’s exposed brain within the operating room (OR) to the pre- operatively acquired neuroanatomical images has become commonplace. More specifically, surgeons can use a pen-like stylus to point at a specific feature on the patient’s brain tissue and see where that tissue resides on the neuroanatomical images as facilitated by an interactive display. One detriment to this process is when the patient’s brain deforms due to common surgical manipulations. As a result, the alignment between images and the patient’s physical brain becomes compromised and surgical error could ensue. Over years 1-7 of this award (initial submission & first renewal), we have demonstrated that intraoperatively acquired cortical surface geometric data can be used to: improve image-to-patient alignment, measure brain deformations during surgery, and drive a computational approach to brain shift correction during image-guided neurosurgery. In this application, we take the final step of extensive intraoperative validation and independent testing. The hypothesis to be tested is that computer models, cortical surface geometric data, and tracked stylus digitization technology when used to compensate for deformation during image-guided brain tumor surgery can predict the locations of eloquent brain surround pathology such that this approach is an effective surrogate to intraoperative magnetic resonance (iMR) imaging. The specific aims to accomplish this are to: (1) integrate a novel computer-vision based approach to surgical field digitization within the surgical microscope and commercial guidance environment such that acquired data can drive a computer model-based approach to correct displays for deformations, (2) conduct a 20 patient retrospective validation study with independent collaborator Dr. Alex Golby of Brigham and Women’s hospital comparing the results from our cortical surface deformation driven compensation pipeline to that acquired by the “gold standard” iMR imaging approach, (3) conduct two prospective 20 patient studies at Vanderbilt and the Brigham respectively, and evaluate intraoperative workflow, as well as the efficacy of corrected displays at institutions wit and without the presence of the iMR alternative. With respect to the importance of this work, in large part, the use of image-guided surgery for surgical resection in soft-tissue organs has been confined primarily to the cranial environment with the common understanding that ‘brain shift’ is a problem. With the resolution of deformations by this low-cost minimally encumbered solution, the ability to translate image-guided surgery to other soft- tissue organs could become commonplace. Furthermore, the approaches herein are inexpensive when compared to intra-operative imaging methods (e.g. MR), and scalable, i.e. capable of widespread adoption. This application could be seminal in providing the needed surrogate for the wider populations of patient that could benefit from improved ‘deformation corrected’ guidance but may not have access to iMR facilities.